
Access this comic as a PDF or read below.
Comic Takeaways
- Comic-making can be a tool used not only for self-reflection and communication, but also for new discovery and self-transformation. The act of giving the hand (and not only the brain) an active role in the therapeutic process can allow the distance needed to gain a new, unexpected perspective.
- Comics can function as a component of universal design for learning (UDL) in therapeutic and other clinical settings, offering the client a format of interest to engage with the therapeutic process in a more effective and meaningful way.
- While the comics here focus on the use and effects of cartooning for the recipient of therapy, they also suggest some potential benefits for practitioners, such as aiding their learning about clients and enabling more interactive therapeutic sessions.
- In addition to therapeutic comics themselves, rhetoricians of health and medicine might study the process of creating and using such comics, and the impacts of this, as a form of patient experience design.
Artist Statement
In 2022, I had a new epiphany related to graphic medicine. I had struggled for years to find an approach to therapy that truly worked for me. Although I had tried different things as a recipient of therapy, these had never resulted in long-lasting or effective changes in my life. I thought about trying art therapy but also kind of figured that is what I already did (though in a “self-study” way) daily—creating art to process things. And this had been very effective for me, even when talk therapy was not. So instead of seeking to create art during therapy sessions, I inquired about using my cartoons (which are already a form of graphic medicine) as a starting point for my therapy sessions. This allowed me to not only draw and think about facets of my life, but to then process them further with another person—an element mostly missing in my previous therapy experiences. Somehow, using the drawings as a jump-off point made it easier to describe these experiences to another person (the therapist), which I had always struggled to do in the past with words alone.
This worked pretty well for a while, and I was pleased with the result. I was pushing myself to explain more deeply the concepts I had drawn, leading to fruitful discussion and deeper processing. But then another issue emerged: what was my therapy “homework” if I was already doing the artwork in between sessions? Although the act of drawing cartoons has many benefits, I realized I needed a way to push my brain a bit further. Because typical worksheets and exercises were never quite right or me, I decided to try something new in between sessions: drawing responses to my own cartoons, as a way to open my brain up to the possibility of change.
Here’s how this new method works for me: I choose a cartoon I have drawn in the past which depicts a scenario or situation I have been struggling with, or which I would like to further explore. I then draw a cartoon that is a response to the original cartoon, wherein I make something different happen on the page. The response cartoon does not have to be an attempt at a solution. Rather, the goal is to take something about the original cartoon, put it onto the page, then make something different happen. That’s it. Just create an opportunity for change within the same scenario.
It is important to mention that this cannot be decided ahead of time. This method of response cartooning is based on the premise that cartooning is powerful because it allows the hand (and not the brain) to lead the way. While the original cartoon shows an existing truth (or something that is), the response cartoon shows a possibility (or something that could be).
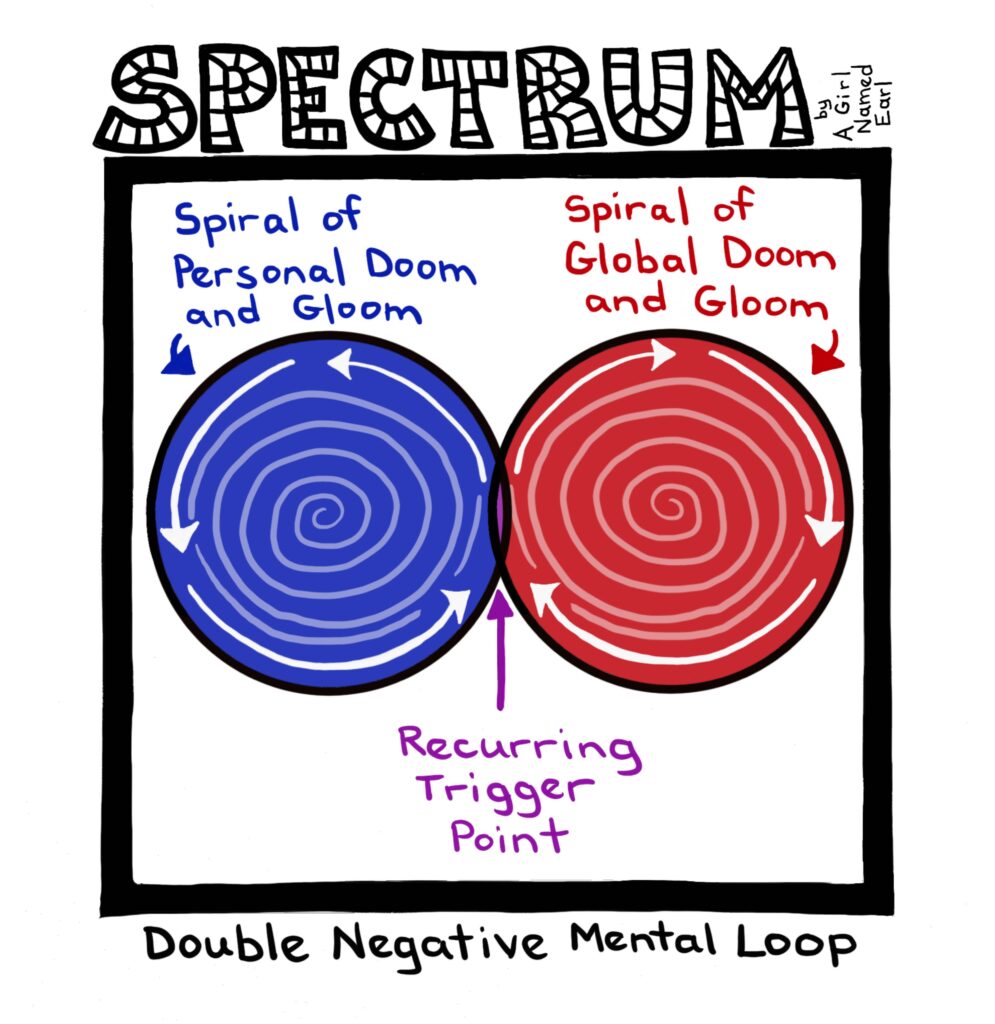
The first cartoon I chose for this exercise was a SPECTRUM cartoon subtitled “Double Negative Mental Loop.” This cartoon depicts a scenario that had kept me stuck in a difficult place for over a year. Something would trigger a negative thought or anxiety—either about my own personal life or about the world at large—and then both of those realms would go into a tailspin of negative thoughts. It was exhausting to experience and difficult to describe to others.
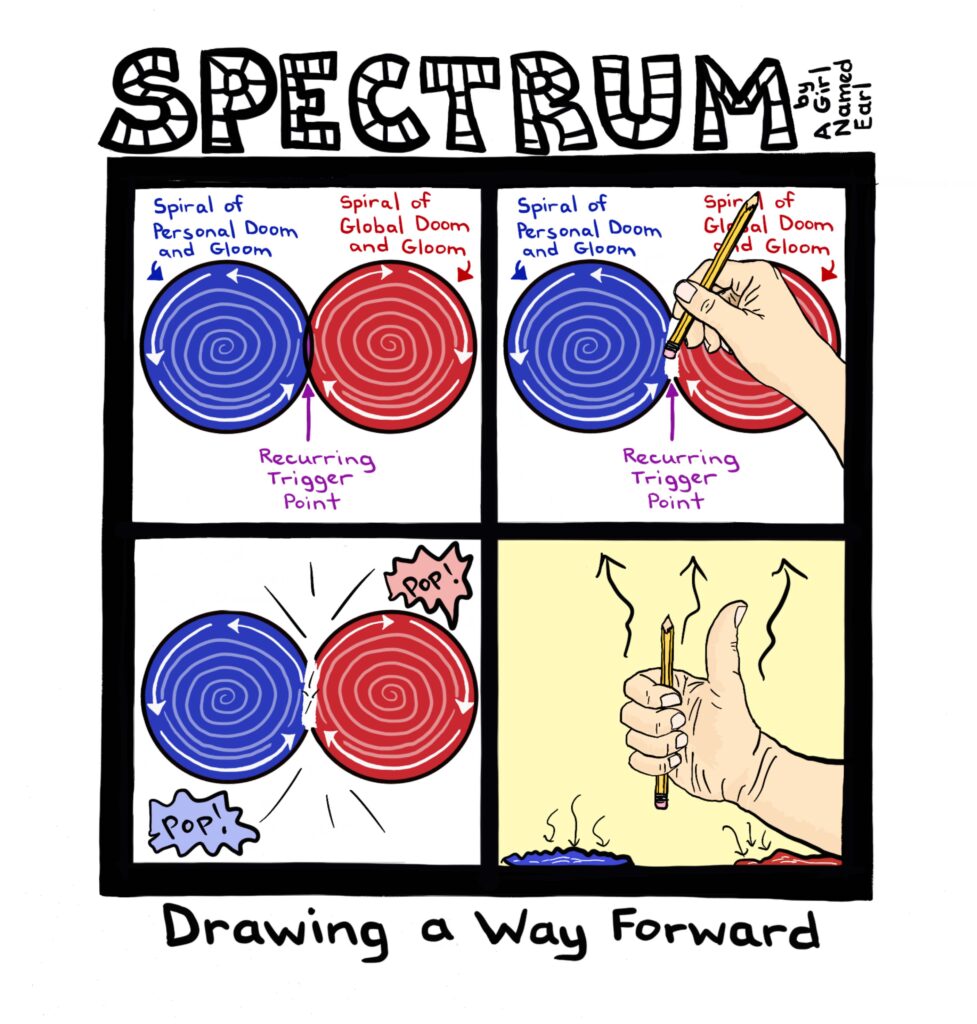
For the response cartoon, I started with the original image from “Double Negative Mental Loop,” but then left space for three more panels. I did not know what would fill those panels, but I just let my hand start drawing its own response. The result was that a hand (depicting my own hand, as the artist) broke through the fourth wall in panel 2 and erased the trigger. This resulted—in panel 3—in the popping of the two negative mental loops. In the final panel, the artist hand is giving a thumbs-up, showing that the double negative mental loops have been deflated.
Now clearly, this response cartoon did not solve any problem in real life. It also did not depict something that had actually happened. Had I found a way to remove the trigger in question? I had not. Had the negative mental loops exploded or disappeared in real life? They had not. So why did this exercise feel so effective? What did it create or allow that was different from before? I wasn’t sure, but I knew that something significant had occurred. It was not like a magical cure, but it was definitely an action—a step forward. And so I continued.
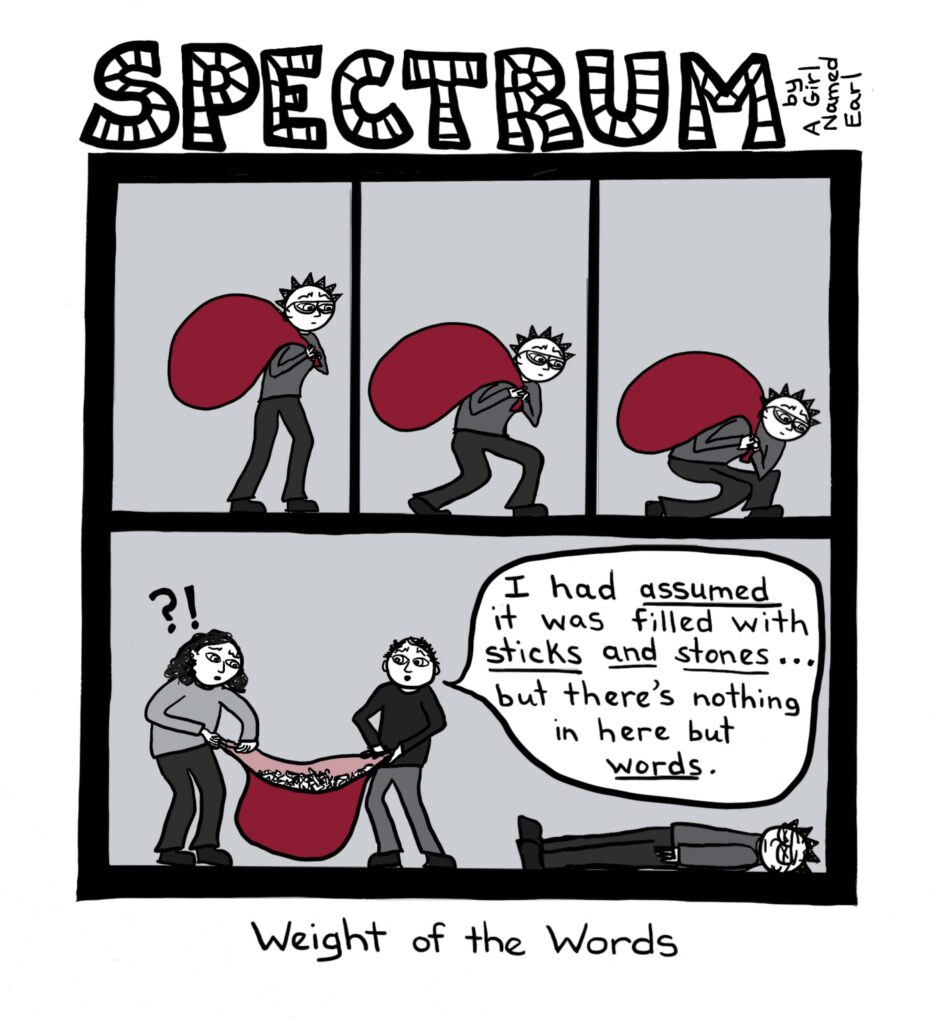
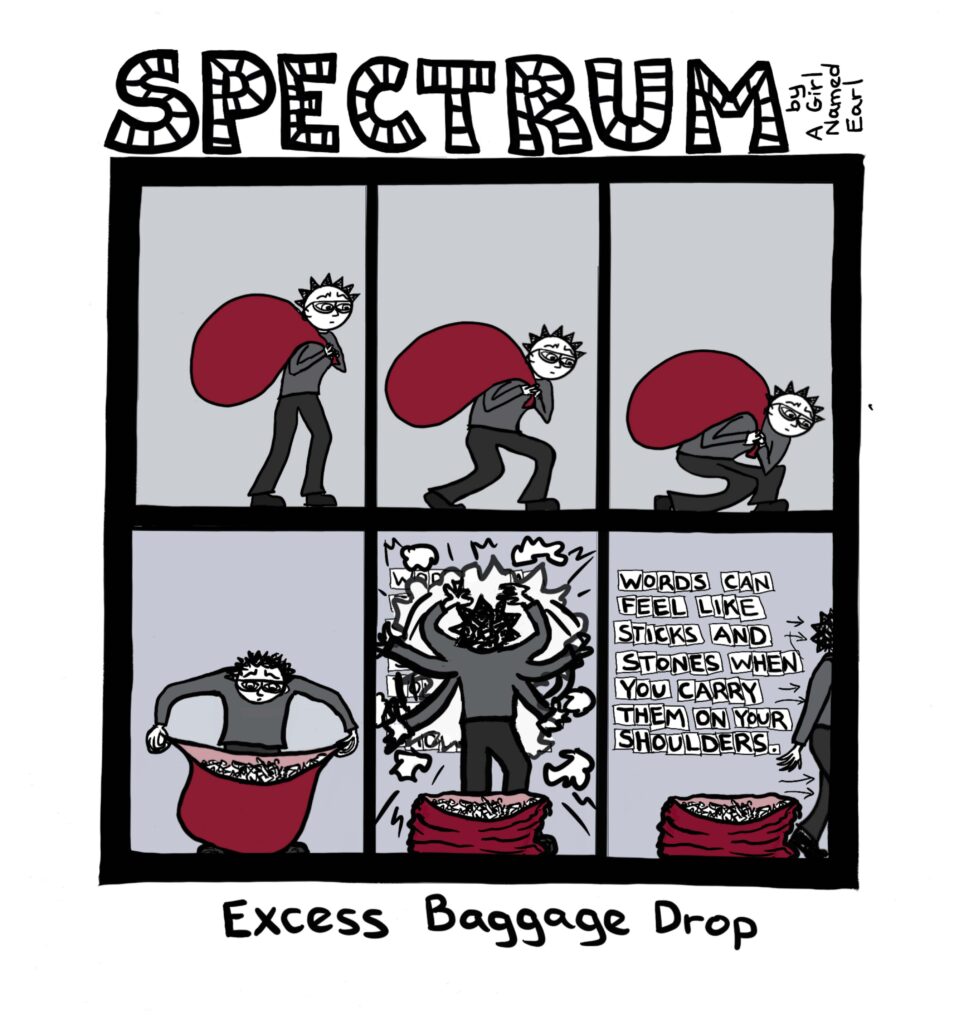
Another cartoon I had drawn, depicting a scenario of feeling stuck, was called “Weight of the Words.” In this cartoon, the character is shown carrying a bag on their shoulders, and ultimately lying flat on the ground as a result. Passersby inspecting the contents of the bag are surprised to find it had only words inside. In the response cartoon, I started the sequence with the same three panels, but then a change occurred. Instead of continuing to carry the bag, the character opens it and looks inside, seeing that it is filled with only letters and words. They then assemble some of the contents to write the message “Words can feel like sticks and stones when you carry them on your shoulders.” In the last panel, the character is seen exiting the area, leaving the sack of words behind.
I eventually recognized that this process allows something to happen in my brain, enabled by something happening on the page. It does not seem to matter whether that change (the one that appears on the page) has happened in real life. It is simply the act of letting my hand explore another way forward, and then seeing what happens. Somehow, it frees up my mind to remember that if it can get stuck, then it can also get unstuck.
I have now been engaging in this practice for about a year. The process of drawing through my issues has had significant effects on my mental health, both in the moment and in the longer term. While I am drawing, I feel a sense of relief. I can temporarily let go of the stress and uncertainty of the unknown. In that moment, it feels as though I am handing over the reins to the process, letting it take over for a while. I can slow down and go into a different state—as more of an observer or passenger. Once I finish a drawing and look back at the page to study what has emerged, I feel a deeper understanding of the place where I have been stuck, as well as a possibility of moving beyond that place.
Now that I have engaged in this process for a while, I can feel the longer-term effects. Over time, this process has offered me a sense of control over those issues. They have not magically disappeared, but they are also not insurmountable and impossible to sort out. I still have to work through them, but the distance of perspective I can now bring quiets the feelings of panic and allows me to recognize and study the situation. I am able to react more with logic and contemplation, where before I could only manage a fight or flight response.
It could be tempting to think of this application of graphic medicine as being some original innovation, but it is really just an example of something we should all be considering more in health practices: universal design (UD) and universal design for learning (UDL). Healthcare is a learning process—both for the practitioners and for the patients/participants. Problem-solving is a big part of the equation, especially in mental health care. And problem-solving is not about static protocols—even when those protocols may be considered “evidence- based” or “time-tested.” Care is dynamic in nature. It is about exploring an assortment of possible tools, resources, and pathways. Because each exploration can lead to more insight and transferrable knowledge, it makes sense to consider the components of UDL in interactive treatment protocols.
UD is an approach that considers the many different ways that people might use a given space, process, or environment (Steinfeld & Maisel, 2021). Unlike individual accommodations or separate access strategies, UD attempts to include everyone in the early design stages of spaces and processes in order to increase overall access and usability. Similarly, UDL is an approach that considers the many different ways people receive, process, and relay information and incorporate that into teaching and learning methods. This helps make learning more accessible to people of all backgrounds and learning styles. One important element of UDL is recruiting interest for the learner. If a learner is able to tie new information to current subjects of interest, they are more likely to grasp new ideas and to retain what they are exploring (CAST, 2018).
Though UDL is typically discussed in classroom settings, it can also increase access, flexibility, and equity in the context of clinical practice (Eisenbaum et al., 2022). In therapeutic contexts, the practitioner should not be seen as the keeper of all the knowledge, who then imparts that knowledge onto the client. Rather, the practitioner is a guide who helps the client explore possibilities within themselves.
People often come into the therapeutic space with their own tools and resources on hand, only to set them aside and wait for the practitioners to give them a new tool that might change everything for the better. And perhaps sometimes it goes that way. But it can also be useful to identify the interests and tools already present, then lean into that familiar territory as a core part of the interactive process. That is what happened with me with the use of cartooning in therapy. For me, this was a way into the therapeutic process. Comics and creative expression were my familiar tools and area of interest. Building on that method and that interest has been a good way for me to take in, process, and relay back information throughout the process of therapy. When graphic medicine and UDL come together, they can create more opportunities for meaningful participation and understanding between practitioners and clients in a wide range of clinical settings. The important thing is to recognize what each person is bringing to the table, and to put those tools to use in creative, collaborative ways.
References
CAST. (2018, August 31). UDL: The UDL guidelines. Cast.org. http://udlguidelines.cast.org
Eisenbaum, Elaine, et. al. (2022). Serving clients with developmental disabilities in clinical practice: Utilizing a universal design framework. Social Work in Mental Health, 20(4), 418-431.
Steinfeld, Edward, & Maisel, Jordana. (2012). Universal design: Creating inclusive environments. John Wiley & Sons, Inc.
Click on an image below to open a larger version.
Artist Bio
Erin Fitzgerald (she/her/they/them); a.k.a. A Girl Named Earl) is a multi-directional artist from Kentucky. Her current cartooning projects include a single-panel series focusing on neurodivergence and queerness (“SPECTRUM”), and a wordless graphic memoir-in-progress about mental health/care (“InQuest”).
To Cite
Fitzgerald, Erin. (2023). SPECTRUM [comics and artist statement]. Rhetoric of Health & Medicine, 6(4), http://medicalrhetoric.com/graphicRHM/home/archive/column-1/fitzgerald/